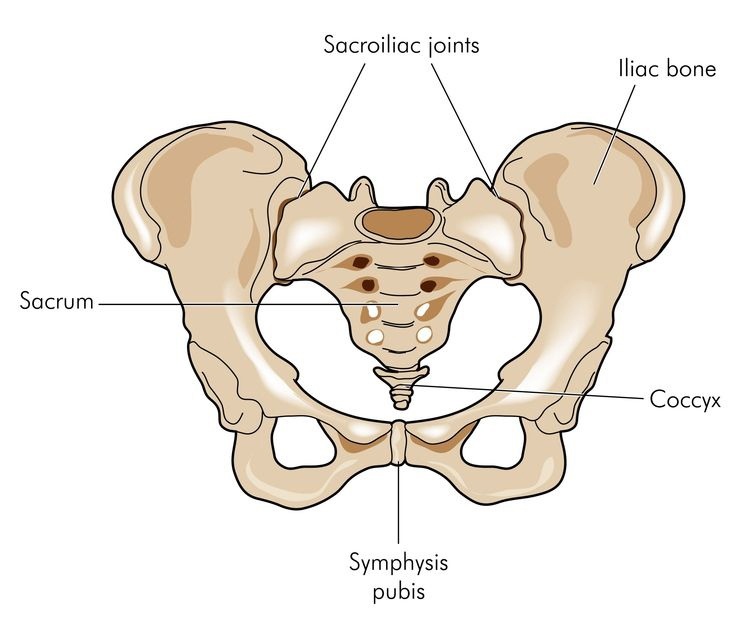
As the name suggests this joint is formed by the union of two separate bones, one being the lower part of the spine (the sacrum), and the second, being one of the three bones which make up the pelvis (the ilium). Hence the L-shaped sacro-iliac joint (SIJ).
The two different surfaces are covered with different types of cartilage. Until puberty the surfaces are flat, then as muscle mass and bone density increase these surfaces become rougher, forming interlocking ridges. This feature is vitally important for the normal functioning of the joint, as it serves to increase the level of friction and thereby improves the joint’s stability.
Covering the surfaces of the joint are a network of dense ligaments whose function is to hold the opposing surfaces together and further enhance joint stability. Running over these structures are several groups of muscles which when contracted, work to tighten still further the interlocking surfaces of the joint, thus preventing excessive movement and dysfunction.
Biomechanically, this area is a bridge between the lower limbs and the trunk and as such responsible for controlling large amounts of movement and stresses produced in either the legs or the upper body. The joint can move approximately two degrees in all three planes under normal circumstances, but when unequal movements occur between the two sides of the joint, pain and dysfunction can result.
In the past, circa. 1900, the sacro-iliac joint was thought to be main source of low back pain and sciatica. This assumption was supplanted in 1934 by evidence suggesting that the intervertebral discs were the main source of pain.
Nowadays as a result of more than 50 years of investigation, more accurate figures have come to light. These show that 30% of low back pain originates from the sacro-iliac joint, and in pregnant women it is the cause of 50% of lower back pain.
Common symptoms associated with dysfunction of this joint are:
* pain directly over the area
* dull buttock
* groin or posterior thigh pain
* or subjective heaviness
* deadness or dullness of the limb
Certain movements, such as turning over in bed or walking up stairs can trigger pain. A history of one sided work posture or unequal stresses (for example, with a sport like fast bowling) can alert the physiotherapist to the cause.
Pain around the lower back can be due to damage to several different structures. A physiotherapist will generally examine the lumbar spine, the sacro-iliac joint and the hip, to discover which of these structures is causing the problem. These tests are a combination of observation of body structure and associated physiological movements and various tests of joint stability and muscular function.
Treatment aims to restore stability and reduce the demands for mobility on the unstable side. This involves mobilisation of adjacent segments – the opposite SIJ, the spine and hips for example, and re-education of muscular support and use. This involves retraining of the integrated and co-ordinated actions of the four major muscles, which bring the muscles back to the normal level of functioning.
In conclusion, SIJ problems cause almost half of all lower back problems and can be treated successfully by muscle mobilisation and re-education during physiotherapy.